While I was in France, I hit my 20-year anniversary with type 1 diabetes.
In October 1998, I was a graduate student at Eastern Michigan University. I’d been really thirsty for a while, was having to pee all the time, and had turned into a Very Grumpy Jim. I also lost about 20 pounds, dropping to around 130ish.
My father is also type 1, so I was somewhat familiar with the disease, and had an idea what was happening to me. I went home and borrowed dad’s glucose meter, which said my blood sugar was too high to read. And that day — Halloween of 1998 — off to the hospital we went.
I’ve blogged about this from time to time over the years. I started out taking multiple shots a day and using a glucose meter that took 30 seconds to process my blood sample. A little while later, I switched over to an insulin pump. The meters got faster, smaller, and started using smaller blood samples.
I changed my diet in some respects — the biggest change was probably switching away from sugared pop — but I don’t have a rigid diet or meal schedule. Instead, I check my blood more often and fine-tune with my insulin as needed.
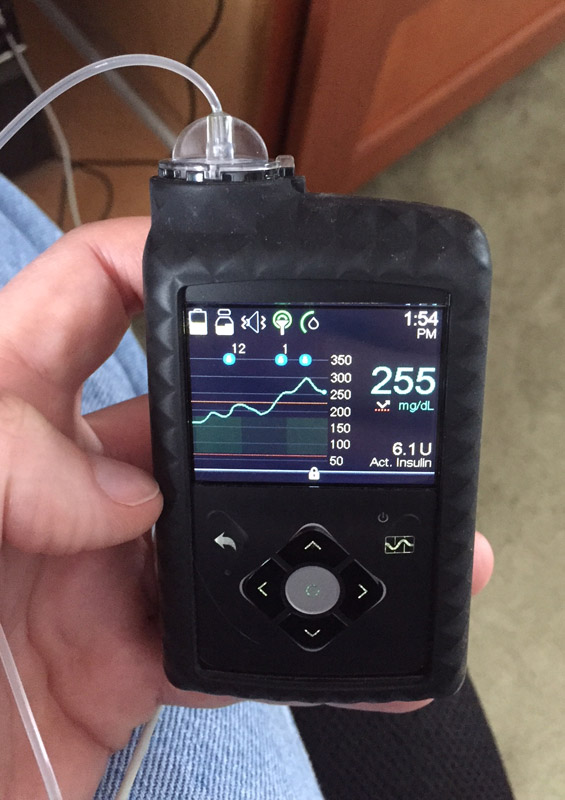
Earlier this year, I upgraded to a continuous glucose monitor, which gives me rough real-time data about my blood sugar. I still need to manually test my blood a few times a day to calibrate and double-check the CGM. My current meter is the size of a large USB thumb drive, and automatically sends my blood glucose reading to the pump. It also buzzes and beeps at me if my sugar starts to drop too low, which is both reassuring and obnoxious.
I’ve been pretty fortunate so far. We haven’t seen any direct complications from the diabetes. I’ve had a few other conditions come up that tend to be more common in diabetics — a minor thyroid malfunction, Dupuytren’s disease (which will require hand surgery in the coming years), and a bout of Peyronie’s disease (which is more common among people with Dupuytren’s, but may not be directly linked to the diabetes…) Annoying as these have been, they were all manageable/treatable, one way or another.
I’m also lucky to have very good medical insurance, which has covered most of the cost of my supplies and medications. A lot of people aren’t so fortunate, having to pay hundreds of dollars for each vial of insulin. Some end up rationing their insulin, which can lead to hospitalization and/or death. The American Diabetes Association has more information on their Make Insulin Affordable website.
I’ve learned two big lessons about the disease over the past two decades. (So I’m averaging learning one lesson every ten years. I never claimed to be a quick learner.)
1. The worst thing you can do is ignore or neglect the disease. A lot of the side effects happen over the long term. If I blow off checking my blood sugar for a few days, or let my sugar get out of control for a bit, it’s not likely to kill me right away. I might not even notice any immediate problems…for a while. Unfortunately, by the time you do notice, you’re likely to be facing major medical complications.
A family friend got into trouble with out of control type 2 diabetes. She needed a kidney transplant, among other things. My father used to play racketball with a man who lost a foot to uncontrolled diabetes.
It’s a pain in the ass having to manage this thing every single day, but it’s a heck of a lot better than the alternative.
2. There’s no such thing as perfect control. Yesterday I had a sandwich, granola bar, and yogurt for lunch. My blood sugar jumped into the 200s and insisted on staying there for much of the early afternoon. Today I had the exact same lunch. I took the exact same amount of insulin. My blood sugar is currently 112.
Why the difference? Heck if I know. Maybe my activity level was different? Maybe I was more stressed? Maybe the diabetes fairy rolled a natural 20 and got a critical hit on my blood sugar yesterday.
There’s a lot I can and should do to fine-tune my control, but there are too many variables to control them all, and sometimes stuff happens that just makes no damn sense. So you do the best you can. Talk to the doctor for ideas on how to improve control. But also recognize you’re not going to achieve perfection.
#
Having inherited this thing from my father, I’m worried about passing it along. Dad and I both became diabetic at age 24. Both of us were in grad school, too. Ergo, I’ll make sure my kids don’t go to grad school until they’re at least 25. Problem solved!
Or not. But given how far the technology has come just in the past 20 years, let alone the 44 since Dad was diagnosed, I’m hopeful that when and if one of my kids comes down with it, we’ll have gotten the disease mostly under control, if not cured outright.
And on the day we do cure this thing — assuming I’m still around — I plan to celebrate with the biggest hot fudge sundae.
Mirrored from Jim C. Hines.
 Taz: LOOK OUT! I WILL SAVE YOU FROM THE IMPROBABLY SKINNY SNAKE THAT WAS BITING YOUR BELLY!
Taz: LOOK OUT! I WILL SAVE YOU FROM THE IMPROBABLY SKINNY SNAKE THAT WAS BITING YOUR BELLY!
 Let’s start with a picture I’ll call Jim’s Collection of Stabby Things. On the left is a typical insulin syringe. I keep some around just in case I ever have trouble with the pump.
Let’s start with a picture I’ll call Jim’s Collection of Stabby Things. On the left is a typical insulin syringe. I keep some around just in case I ever have trouble with the pump. again last night. I removed the old set and checked to see if that site was bleeding. It wasn’t. So I finished prepping the new infusion set for my pump, looked back, and there was a tiny smear of red on my shirt.
again last night. I removed the old set and checked to see if that site was bleeding. It wasn’t. So I finished prepping the new infusion set for my pump, looked back, and there was a tiny smear of red on my shirt. The nice thing is that after I went to the hospital, I felt better within a day or two. Insulin is amazing stuff. I had no idea just how bad I had been feeling until I was better.
The nice thing is that after I went to the hospital, I felt better within a day or two. Insulin is amazing stuff. I had no idea just how bad I had been feeling until I was better.
